

Twitter Censorship, Vaccine Risk, and Myocarditis Mumbo-Jumbo

I received this email from Twitter at 12:56 PM, Thursday, April 7, in response to a Tuesday tweet of mine:
Here is my transgressive tweet in the context of the thread as it displayed on Friday, with Twitter’s warning (It seems to have disappeared since):
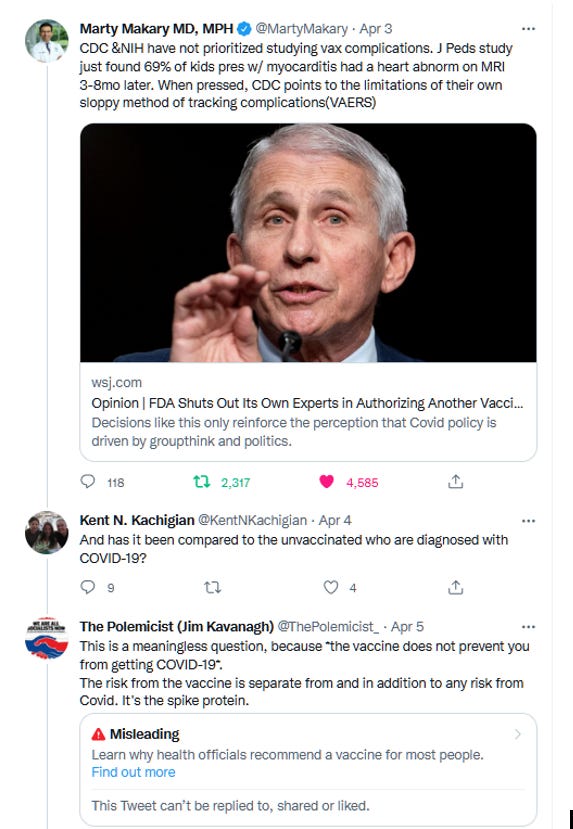
The important thing here is, of course, the substance of my tweet, which is neither “misleading” nor “potentially harmful” but true. This incident prompts me to address one of my pet peeves in the vaccine mandate debate (because here, as always, the issue of the vaccine always becomes an issue of a mandate): the conversation in which stating the fact that the mRNA vaccines carry an elevated risk of myocarditis (especially to young males) is met with the riposte that “But Covid carries a greater risk!”—delivered, and usually accepted, as a mic drop that shuts down the concern over the vaccine.
The signal example of this occurred in Joe Rogan’s conversation with Australian media personality Josh Zepps, where, as Yahoo News reports it:
Rogan said he had read reports that showed there was an “adverse risk” of myocarditis – an inflammation of the heart muscle – among 12-17-year-olds who received the vaccine.
Zepps countered by pointing out that there is an increased risk of myocarditis from Covid-19 among the same age group that exceeds the risk from the vaccine.
Here’s Rogan’s tweet containing the relevant clip:

So, Rogan accepted Zepps’s rejoinder as conclusive, as a “gotcha” that made him “look dumb” for his concern about vaccine-induced myocarditis, and the incident became a prime exhibit in the ridiculous campaign to deplatform Rogan.
Lesser-known examples of this argument include this, from Joshua Frank’s attack on RFK, Jr.:
like so many of RFK Jr.’s blatant lies, the bogus claim that mRNA vaccines will give you lethal heart trouble, is easily debunked. (Yes mRNA vaccines can cause heart inflammation, known as myocarditis, primarily in younger men, but these incidences are very rare and typically mild. In reality, far more covid infections cause myocarditis, along with a host of other ailments, some lethal, like stroke, arrhythmia and kidney injury. A pre-print study also found that myocarditis is by far more common after covid infection than vaccination in teen boys, 450 cases per million infections vs 67 cases per million vaccinations.)
Let’s, for the moment, ignore all the contrary evidence—i.e., “that in younger males receiving a second dose of mRNA-1273 vaccine, the risk of myocarditis was [14 times] higher following vaccination than infection”—and accept, for the purposes of this discussion, the proposition that in every category of persons there’s a higher risk of myocarditis from being sick with Covid-19 than from getting the vaccine. OK. So what?
That’s an interesting factoid, but it has nothing to do with whether anyone should take—let alone be forced to take—the vaccine, because the vaccine does not prevent infection. The risk from the vaccine is separate from, in addition to, and unmitigated by, any risk from Covid.
The risk from infection cannot eliminate or be eliminated by the risk from a drug that does not stop infection. With the vaccine, there are two risks, and neither eliminates the other.
Whatever the risk from infection, it cannot be cited to cancel out concern for the risk from the vaccine, which does not prevent infection. Citing a higher risk of myocarditis from Covid than from the vaccine is an argument against getting Covid, not an argument for getting the vaccine—although that’s exactly the implication that is being made, and widely accepted. It’s no different, logically and scientifically, than saying: “If you eat bananas, you’ll have an increased risk of myocarditis, but if you get Covid you’ll have an even higher risk. Therefore, eat bananas.” There may be good reasons to eat bananas, but it’s not to avoid myocarditis.
An article in Israel National News. based on a JAMA study, sums it up quite well: “New study: 133x risk of myocarditis after COVID vaccination. Comparisons with myocarditis rates following infection now irrelevant as vaccination no longer prevents infection.”
What one should focus on here is what the common element is in both bananas vaccines and Covid that induces myocarditis. And it’s been well established what that is: the spike protein—which, as detailed in reports by scientists at UC San Diego and the Salk Institute and the University of Bristol, is “alone enough to cause disease,” “has a major damaging effect on the vascular cells” and “binds to cells…which line the small vessels of the heart…trigger[ing] a cascade of changes which disrupt normal cell function” and can cause all those “other ailments” Frank mentions.
That would be the spike protein that mRNA vaccines make your cells produce, which is why there is a risk from the vaccine as well as from the disease, and why it's perfectly reasonable not to want to take a drug that turns your body into a spike protein factory and will not stop the disease from doing so either. Two risks are not better than one.
If you take the vaccine, you have whatever higher than normal risk of myocarditis the vaccine gives you—whether you get Covid or not; if you then get Covid, you will then have whatever higher risk of myocarditis the disease gives you—whether you’ve had the vaccine or not.[1] And many, many people, especially young people, who get vaccinated are not going to get Covid.
Indeed, Joe Rogan’s mistake was that the Guardian article he was relying on was not about whether the relative risk of getting myocarditis from the vaccine versus getting it from Covid; it was about whether young males have a higher risk of getting myocarditis from the vaccine than of getting Covid. And it found, based on a UC study, that they do.
That’s a point that the other New Scientist article Rogan and Zepps then pulled up, which was about the relative risk of vaccine-induced vs. Covid-induced myocarditis, does not address or refute. And it’s an important point. Vaccine mandate proponents love to emphasize how “rare” the incidence of vaccine-induced myocarditis is, as a way of dismissing concern about how less rare than normal it is. They never mention, let alone emphasize, how more rare it is for young people to get Covid—and therefore how many more young people are put at myocarditis risk from the mandated universal administration of the vaccine than from Covid. Because their object is to pitch the mandatory vaccine program, not to give a clear picture of all the risks.
So, the Rogan-Zepps conversation was not one in which Zepps pulled a “gotcha” on Rogan, but one in which both look kinda dumb for not recognizing that they were talking about two different things.
Objection to vaccine mandates is not based on whether myocarditis (or any other adverse event) risk is higher from the vaccine than from Covid, but on the fact that there are risks of serious harm from the vaccine, that the vaccine does not prevent one from getting or transmitting Covid, and that, therefore, the decision about which set of risks to take with one’s body should be one’s own.
(It is astounding that there is any controversy about this elementary ethico-scientific logic on the left.)
Let’s be sure not to accept, for the purpose of making vaccine mandate supporters’ arguments easier, the notion that myocarditis is not serious. Like the word “rare,” “mild” is used to dismiss concern about a serious condition that causes permanent damage to the heart muscle, which does not regenerate. Myocarditis, especially among young people, is a serious adverse event, whether it’s caused by a vaccine or a disease. The impulse to diminish concern about it because it arises from the vaccine is not driven by “science.”
As doctors wrote in a cardiology journal in 2015, before the media and medical bureaucracy was engaged in, and had confected a fictional political impetus for, selling mRNA vaccines:
Clinically, myocarditis can manifest as acute heart failure, ventricular arrhythmias, or cardiogenic shock, and is associated with substantial morbidity and mortality.5 Children diagnosed with acute myocarditis have only a 60% likelihood of transplantation-free survival at 10 years.6 Myocarditis has been linked as the cause of sudden cardiac death in young adults in up to 12% of cases, and identified as the cause of dilated cardiomyopathy in 9% of patients. [my emphasis]
That science did not change. As the cardiologist of a 14-year-old boy with vaccine-induced myocarditis says: “No case of myocarditis is ‘mild.’ That’s like saying a heart attack is mild.” Myocarditis changes a young kid’s and his/her family’s life. Here’s Emily Jo, the mother of that 14-year-old boy:
Jo said…The Centers for Disease Control and Prevention (CDC) said it was very rare and mild.
“What they didn’t explain is that mild means hospital care and follow-up care indefinitely.”…
“I think another thing parents need to understand is that myocarditis is not covered under the National Vaccine Injury Compensation Program, and the Countermeasures Injury Compensation Program only covers if you’re incapacitated, wheel-chair bound or dead. We have incurred thousands and thousands of dollars in medical bills. We have insurance but they don’t pay all. It does not account for tests down the road that we still have to get.”
You do not get to dismiss these devastating concerns about a condition that requires a heart transplant for most children within 10 years and demands hundreds of thousands of dollars in lifetime medical care, with “mild.” Any—especially any “leftist”—vaccine mandate supporter should be ashamed of trying to do so. And none of them would—in fact, they’d all be constantly emphasizing how terrible it is—if myocarditis was only a risk from the disease and not the vaccine. I dare anyone to deny that.
Then again, any “leftist” should be ashamed of supporting policies that force people—in order not to be fired from a job, expelled from school, and exiled from social life—to take a novel gene therapy treatment that doesn’t prevent infection or transmission, has serious known short-term and unknown long-term adverse effects, induces your cells to produce a spike protein that “triggers a cascade of changes which disrupt normal cell function," and will have to be re-administered every few months, without at the very least conditioning that support on full compensation for the harms caused to people by the drug they were forced to take. I dare anyone to make a left argument otherwise.
By now, it’s obvious that vaccine mandate policies were based on an anti-scientific program of deception, censorship, and data manipulation and concealment, for the main purpose of assuring the tens to hundreds of billions of dollars in Pharma profits that were, and will continue to be, successfully captured. It was also built on the credulity of otherwise intelligent people whose critical thinking capacity about such matters evaporates in the harmless-magic-bullet ideology we have all been inculcated with regarding vaccines. The elementary logical and scientific flaw in their riposte about the vaccine’s myocarditis risk is one small element of this. The fact that it endures is a testimony to how tenacious that ideology is, and how stubbornly even the most intelligent people will resist coming to terms with how thoroughly they were played.
[1] There is no evidence I know of that those who are vaccinated have a lower risk of myocarditis when they get Covid, if they have escaped the risk from the vaccine, than those who are not vaccinated. Even if there were, it would not eliminate the risk from the vaccine, which applies to all vaccinated persons, whether they get Covid or not.
It would be very hard to establish that definitively, in a way that would eliminate all other variables. To do so would certainly require a rigorous comparative study of vaccinated and unvaccinated populations—and vaccine salesmen (Pharma and the medical bureaucracy) are loath to do that, for any vaccine.
The only thing that comes close is a study of Covid patients that tried “to eliminate any putative contribution of potential vaccine exposure to the outcomes of myocarditis and pericarditis,” splitting its cohort via certain rules that are unclear to me and “conduct[ing] two analyses.” It stated, in decidedly non-committal terms, that: “The results suggested that COVID-19 was associated with increased risk of myocarditis and pericarditis in both analyses.”
Addendum (July 7, 2022): There is a study now, of 196,992 adults that shows: "Post COVID-19 infection was not associated with either myocarditis…or pericarditis… We did not observe an increased incidence of neither [sic] pericarditis nor myocarditis in adult patients recovering from COVID-19 infection."
You can also make a one-time donation via PayPal, Venmo, or Cash App. Thanks for your support!